
Risk calculator developed with data from 200,000 UK Biobank participants estimates someone’s likelihood of becoming ill from excess body fat.
Summary
Researchers have found a way to predict someone’s likelihood of developing 18 conditions related to excess body fat, such as diabetes, heart attack and liver disease. The method was developed with information from 200,000 UK Biobank participants and could eventually help doctors to better allocate weight-management medications – based on people’s health risks rather than just their weight.
The disease-forecast score is based on data from 200,000 UK Biobank participants
Combining a few simple measurements can forecast someone’s likelihood of developing 18 complications related to excess body fat, such as diabetes or heart attack. It could help doctors to allocate weight-management medications based on people’s health rather than just their body weight.
BMI: useful but flawed
Having a lot of body fat can make it more likely to develop high blood pressure, narrowed arteries, sleep apnoea and many other conditions. Clinicians have long used BMI – body mass index – to estimate this risk. One reason BMI is so popular is that it’s quick and easy to calculate from someone’s height and weight. But it has flaws: it can’t account for muscle mass, how fat is distributed around the body, or differences between sexes and ethnic groups.
We miss the opportunity to identify people [with high disease risk] early, when we could prevent complications.
Professor Claudia Langenberg, Queen Mary University of London, UK
“[BMI] doesn’t really capture very well how much metabolic risk people have,” explains Claudia Langenberg from Queen Mary University of London, UK. Two people with the same BMI can have vastly different risks of becoming ill from their excess body fat. If we ignore this fact, Langenberg says, “we miss the opportunity to identify these people early, when we could prevent complications”.
Langenberg and her colleagues wanted to find a better way of predicting someone’s future risk for body-fat-related conditions. The team analysed more than 2,000 parameters – from genetic factors and blood components to food preferences and medical history – from 200,000 UK Biobank participants. “That’s amazing that you can do that with the information UK Biobank has,” Langenberg says.
20 parameters predict 18 diseases
Out all the parameters the team looked at, 20 emerged as being the most informative. Among them are basic information including sex and age, some routine tests for blood sugar levels and kidney function, and people’s own evaluation of their health. “It was a pleasant surprise that just by asking someone to rate their overall health, we can gain a lot of information on their future disease risk,” says Langenberg’s co-investigator Kamil Demircan.
When applied to participants from other health databases, the 20-parameter score was better than a combination of BMI, sex and age at predicting 18 diseases ranging from chronic heartburn and gout, to heart conditions and liver disease.
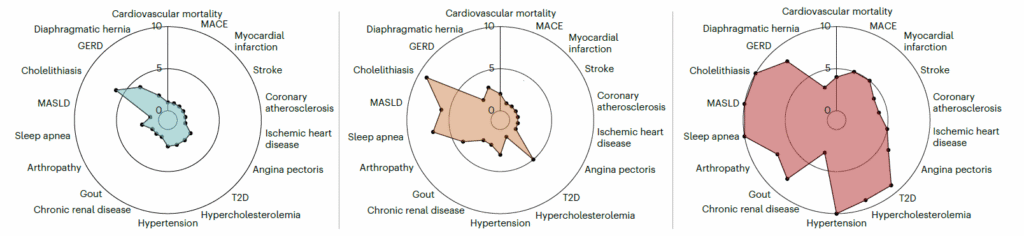
The score revealed that it wasn’t always the people with the highest BMI that were at the highest risk. “It also included individuals with lower BMI levels who had other factors that increased their overall predicted risk,” Demircan explains. These lower-weight, higher-risk people might currently be precluded from treatments such weight-loss medications because the NHS guidelines mostly focus on BMI.
Personalised care – beyond body weight
Finding a method that predicts people’s risk better than weight alone is something the research community has struggled with for a long time, says Francesco Giorgino, a specialist in diabetes and obesity from the University of Bari Aldo Moro in Italy who was involved in the study’s review. “This is interesting research because they were actually trying to provide an answer to this unmet need.”
This is interesting research because they were actually trying to provide an answer to this unmet need.
Professor Francesco Giorgino, University of Bari Aldo Moro, Italy
The results, Giorgino says, show that “you don’t need sophisticated tools: the score is composed of relatively easy-to-obtain measures”. This makes it particularly useful for primary care doctors.
Langenberg points out that before the risk score makes its way into GP practices, it needs to be further optimised for younger people as well as people from ancestrally diverse populations. Giorgino suggests that the score could even be expanded to predict which of the many weight-management drugs would work best for each person.
“We now have effective weight-loss drugs – so how could we prioritise access?” asks Langenberg. “What we’re trying to do is to reduce uncertainty and make that decision process as equitable and as data-driven as possible.”
Related publication
Related publication
- Nature Medicine, April 2026

